@@fareshejazi2297 perhaps 'pat brewer' meant that, through 15 years of lectures/classes, this video had the clearest explanation (compared to pat's lecturer/textbook explanations)
Adding onto his notes in more specificity: The unstable membrane potential for which these pacemaker fibers start is known as a pacemaker potential since the fibers never truly rest at a constant value. This would be the beginning of his stage 4 at about -60mV. These pacemaker fibers contain channels known as I-funny channels, that are different from other excitatory tissues in that they allow Na ions and K ions to both pass. When these channels open at negative values, they allow for a greater influx of Na+ than an efflux of K+. This influx of Na+ slowly begins to depolarize the fibers, which can be seen in his slow incline along phase 4. As the fibers become more inside positive, the I-funny channels slowly start to close. It is at this point, right before the sudden inclination, that a specific set of Ca2+ channels open, allows Ca2+ to move into the fibers and continues to make the auto-rhythmic fibers more inside positive. When the pacemaker potential reaches threshold, a different group of Ca2+ channels open, allowing a sudden rush of Ca2+ into the cell and creating the steep 0 phase. The steep depolarization due to Ca2+ is a key characteristic of pacemaker cells. In other cells, the steep depolarization phase is due to a net influx of Na+. At the peak, these Ca2+ channels close, and slow K+ channels open. The rapid efflux of K+ is responsible for repolarization (his phase 3). This phase is similar to other excitatory cells. Similarly, the small "under shoot" at the end of the steep decline signifies the closure of K+ channels. Among other things, the time it takes for depolarization of pacemaker cells determines the heart rate.
+Crist Gord hi guys, the best results that I have ever had was by using the Anatomy Blueprint Pro (just google it) definately the no.1 course that I've followed.
im really frikkin annoyed now. these videos do a great job explaining how the heart works and what each organelle does but!!!!! for the SA node...calcium rushes in yes? then it slows/stops. then potassium rushes out okay. depolarisation and repolarisation. then what? how does the sequence start again? we are left with the inside of the node having a large amount of calcium and the outside a large amount of potassium.... is there a pump that reverts it all back to normal? or does the next action potential start with POTASSIUM rushing in instead of calcium. this shit is NEVER explained and it confuses the shit out of me. please can someone help.
iabaca Hey mate just saw this and I'm sure you're well past caring (6 months ago). Anyway, it's a bit of a misconception that the ions actually 'rush out' - e.g. potassium ions - to massive degree. What's happening is a change in the open or closed state of the channels. So there actually isn't a huge amount of potassium efflux from the cell - it's just that a lot of potassium channels open, and that changes the driving force or potential - i.e. it becomes more permeable. You're right, it doesn't really make sense that huge amounts of this stuff rushes in and out of the cell all of the time - and for the most part, it doesn't! The other thing that helps think about that is that the extracellular fluid around the cells contains a certain make-up of ions - this isn't constantly changing in massive waves, rather, it stays fairly constant, otherwise it could potentially affect the other cells (if there was a sudden increase in extracellular potassium then all the surrounding cells would have their membrane potential changed, by this logic. However, in cardiac cells the main driver of calcium potential changes (or rather, the degree of calcium channel opening) actually comes from within the SR calcium storage, rather than the extracellular calcium concentration. Just in case you never had this resolved! This website provides a better worded explanation of what I tried to say: www.austincc.edu/emeyerth/mempot1.htm
Armando, I am truly grateful for your videos. Your videos have help breakdown complexing subjects into bite size clear information. You have an amazing way of teaching the material and thanks to your videos I made it through my Pathophysiology course. Thank you again for taking the time to help me and so many who struggle with reading words on a textbook. Thank you again and God bless !
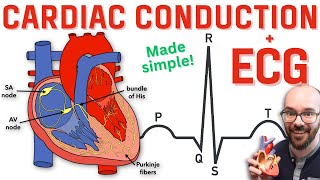
Cmiiw : SA node -> AV node -> Bundle of Hiss -> Purkinjae Fibers Location, SA : Crista Terminalis - Atrium Dextra Posterior AV : Trigonum Koch - near A-V Valve Bundle of Hiss : Interventriculare Ceptum Purkinjae Fibers : spread in Miocard Ventricle
I wonder what sort of student are you and if you have got qualification which is verified by those who are well qualified in this subject not necessarily a doctor or a professor ?
He mispronounced "systole" and "diastole". It should have sounded like "sis-TOE-lee" and "die-ASS-toe-lee". I came to the comments section to see if anyone else noticed that and you were the only one!
very very very very ......... Great work , u have a genius creative mind (prefrontal cortex :P ) that connects all things together in a simple way ,,, I really love this way of looking at things thanks very much man , u are a hero :D
ok...one question right,,,for the ventricle graph..first depolarization means filling the with positive charge..so how is phase0 systolic when there is rapid depolarization....could you kindly explain that as soon as possible
Mr. Richard Adetoye, there's no reply option to your comment so I'll just answer you question here. When you mean systolic, there is contraction of ventricular muscles to push the blood from the ventricles to the pulmonary artery or to the aorta. Depolarization means making the membrane potential to become more positive to make muscle contraction possible. Phase 0 means depolarization of the ventricular muscles thus is part of the systolic phase. Hope this helps.
if you look into the period of the cardiac cycle, there is about 0.3 sec when four chambers are all relaxed and waiting for blood coming into the atrium.I think that area should be shown longer. thank you!
thaaaanx it made alot of sense now..ive been looking for the video next to this one but i couldnt find it could u please tell me how to find it..many thanx
Hi, good catch when you said atrial diastole instead of ventricular diastole. But if you want to add in, the S4 sound should be heard right before the QRS complex. Also when you drew the cardiac myocyte action potential on top of the EKG, shouldn't phase 3 include the T wave instead of ending at the T wave, since the T wave represents ventricular repolarization.
Okay i have a conceptual doubt, you said that in SA node, repolarisation by efflux of Potassium is followed by depolarization of the next Action Potential Cycle. But how do the Calcium ions which entered the cell in the previous cycle go out? Thats a necessary step before the next cycle begins isn't it? Please help me with this i always struggle at this part. :(
This is probably a minor and inconsequential point, but at ~8:50, Armando mentions phase 0 (the steep upward curve) and states that the influx of sodium is the contraction of the ventricles. While this phase of the action potential is the depolarization of the membrane, the voltage-gated influx of calcium (Ca) ions (via the L-type channels) starts at about -40 mV and is more prolonged than sodium influx (lasting throughout phase 2). The Ca ions which influx during this phase trigger a massive release of Ca ion storage from the sarcoplasmic reticulum, which is responsible for ventricular contraction. Therefore, I believe it would be more precise to say contraction of the ventricles happen during phase 2. Source: Pathophysiology of Heart Disease, L. Lilly.
hey man great video. I just have a quick note about the SA node phases. In phase 4, it is true that the L and T types open up channels but they do so after it reaches -40 mV. From -55 to -40 mV is produced by something called a funny channel which is activated by negative membrane potential and this channel bring in Na +. Just wanted to add detail but great video, love your stuff please keep doing what youre doing!
Just one question, in the explanation about the cardiac muscle cell contraction, you say that Na+ stop moving in in phase 1, but then in phase 3 you say both Calcium AND sodium stop moving in, how can the sodium influx stop twice ?
you can't imagine how thankful I am... my exam is tomorrow and I was crying cause I didn't understand it till I found your video and it appears clear like water... thanks you so so much!!!!!!❤❤❤❤❤❤❤❤❤❤❤
The videos are just amazing and so to the point..also Please post some detailed videos on CARDIAC ARRTHYMIAS and ANGINA PECTORIS..and if it has already been made..please provide the link..unable to find it..
Ok... so.maybe I am getting confused between skeletal and cardiac. But wouldn't a repolarization involve an influx of potassium? He says eflux but this doesn't make sense to me cause the whole purpose of membrane potential is offsetting balance between sodium and potassium and a continued eflux of potassium would never allow the membrane to reach resting membrane potential. Thanks
Hey sorry if I'm wrong but what I think is this: Depolarization --> 3 Na influx & 2 K outflux, thus the inner side of the cell membrane becomes more positive resulting in depolarization. Repolarisation means that the inner side of the cell membrane has to become more negative. So we have to pump extra positive charge out of the cell, this way we get a negative inner side of the cell membrane. Thus the Na-K pump pumps 2K out of the cell...K efflux. Hole it helps. :-)
*Hope. The Na-K pump only pumps Na out of the cell and K into the cell. It's a one way pump. Search: Na-K pump conformations. Being in a particular shape of the pump E1 or E2 creates specific affinities to either K or Na. I think, please google and tell me if I'm wrong, that on the inside it can only pump Na inside and K outside.
I'm not sure if I get you question right, but when you say repolarization, you are making the inside of the cell more negatively charged. For you to be able to do this, Ca2+ and Na+ channels should be closed to prevent further increase of positive ions within the cell, and also, there must be a K+ eflux so that positive ions will move out of the cell making it more negative thus repolarizing it.
Thank you for this amazing video but i want to point out about the action potential of the SA node, the action potential peak reaches +10 not 0, otherwise there will be potential difference between the charges if it stops at 0
There is something not clear to be , when you draw a digram of ECG how it can be the distend from P wave to R represent atrial systole ( ventricular diastole ) and the distend from the T wave to P wave atrial systole also. Please if you can make it more explanation to me . Thank you
Mosbah Maryd The atria are in diastole most of the time - atrial systole only occurs during the PR interval. Action potentials fire first which causes the muscle to contract. We start with the heart relaxed, with the atria and ventricles in diastole, both full of blood. The action potential spreads across the atria (P wave) then there is a small amount of time, about 0.2 seconds, before the action potential reaches the ventricle muscle cells (QRS). This small amount of time is called PR interval, and during this time the atria contract, squeezing their blood into the ventricles (atrial systole), and then relax (atrial diastole) and repolarise. The atrial repolarisation can't be seen on an EEG because the action potential (QRS) reaching the ventricles is so much stronger. During the time between S and T, the ventricles contract (ventricle systole) and pump blood into the lungs/body. Ventricles then relax (diastole) and repolarise. The T wave is ventricular muscle cells becoming more negative so they are ready to contract again for the next heart beat. The entire heart is resting in diastole during the time between T and the next P.









LOL - "I hope this isn't too confusing" I've been a cardiac nurse for 15 years and this is the clearest explanation I have ever received!! Thank you:)
mate if you dont understand it after 15 years of working then i dont think it is the explantion fault
@@fareshejazi2297 perhaps 'pat brewer' meant that, through 15 years of lectures/classes, this video had the clearest explanation (compared to pat's lecturer/textbook explanations)
I agree, I watched a ninja nerd video before this and couldn't even last 5 minutes without being confused...
You gave me hope, then you took it away. There is no next video on this topic.
You are the Godfather of modern medicine
I just got back from my physiology finals...and i ACED it...all thanks to you...thank you man :D
Adding onto his notes in more specificity:
The unstable membrane potential for which these pacemaker fibers start is known as a pacemaker potential since the fibers never truly rest at a constant value. This would be the beginning of his stage 4 at about -60mV. These pacemaker fibers contain channels known as I-funny channels, that are different from other excitatory tissues in that they allow Na ions and K ions to both pass. When these channels open at negative values, they allow for a greater influx of Na+ than an efflux of K+. This influx of Na+ slowly begins to depolarize the fibers, which can be seen in his slow incline along phase 4. As the fibers become more inside positive, the I-funny channels slowly start to close. It is at this point, right before the sudden inclination, that a specific set of Ca2+ channels open, allows Ca2+ to move into the fibers and continues to make the auto-rhythmic fibers more inside positive. When the pacemaker potential reaches threshold, a different group of Ca2+ channels open, allowing a sudden rush of Ca2+ into the cell and creating the steep 0 phase. The steep depolarization due to Ca2+ is a key characteristic of pacemaker cells. In other cells, the steep depolarization phase is due to a net influx of Na+. At the peak, these Ca2+ channels close, and slow K+ channels open. The rapid efflux of K+ is responsible for repolarization (his phase 3). This phase is similar to other excitatory cells. Similarly, the small "under shoot" at the end of the steep decline signifies the closure of K+ channels. Among other things, the time it takes for depolarization of pacemaker cells determines the heart rate.
thank you, sir!
Thanks
You added very little, repeated some of what was explained and somehow felt an urge to waste your time.
You got me through my freshman semester of PA school...now you're getting me through my sophomore semester. You rock, man! Thanks!
+Crist Gord hi guys, the best results that I have ever had was by using the Anatomy Blueprint Pro (just google it) definately the no.1 course that I've followed.
+Lucian Lucian SPAM
+Tena Preseđanski SPAM
+Tena Preseđanski SPAM!!!
Whats PA school?
this is by far the best ecg and heart function explanation in history.
Indeed
im really frikkin annoyed now. these videos do a great job explaining how the heart works and what each organelle does but!!!!! for the SA node...calcium rushes in yes? then it slows/stops. then potassium rushes out okay. depolarisation and repolarisation. then what? how does the sequence start again? we are left with the inside of the node having a large amount of calcium and the outside a large amount of potassium.... is there a pump that reverts it all back to normal? or does the next action potential start with POTASSIUM rushing in instead of calcium. this shit is NEVER explained and it confuses the shit out of me. please can someone help.
Yes, ions are always brought back to where they originated from by "ATPase pumps"
okay thanks. atleast somene explains. but damn these pumps must be fast to do this in a fraction of a second
iabaca Hey mate just saw this and I'm sure you're well past caring (6 months ago). Anyway, it's a bit of a misconception that the ions actually 'rush out' - e.g. potassium ions - to massive degree. What's happening is a change in the open or closed state of the channels. So there actually isn't a huge amount of potassium efflux from the cell - it's just that a lot of potassium channels open, and that changes the driving force or potential - i.e. it becomes more permeable. You're right, it doesn't really make sense that huge amounts of this stuff rushes in and out of the cell all of the time - and for the most part, it doesn't! The other thing that helps think about that is that the extracellular fluid around the cells contains a certain make-up of ions - this isn't constantly changing in massive waves, rather, it stays fairly constant, otherwise it could potentially affect the other cells (if there was a sudden increase in extracellular potassium then all the surrounding cells would have their membrane potential changed, by this logic.
However, in cardiac cells the main driver of calcium potential changes (or rather, the degree of calcium channel opening) actually comes from within the SR calcium storage, rather than the extracellular calcium concentration.
Just in case you never had this resolved! This website provides a better worded explanation of what I tried to say: www.austincc.edu/emeyerth/mempot1.htm
This channel is getting me through Anatomy and Physiology. Bless your soul!
I hope you failed
ruclips.net/video/gplKCkQe7qc/видео.html
thank you so much for this video and the image of your notes, so helpful!
Armando, I am truly grateful for your videos. Your videos have help breakdown complexing subjects into bite size clear information. You have an amazing way of teaching the material and thanks to your videos I made it through my Pathophysiology course. Thank you again for taking the time to help me and so many who struggle with reading words on a textbook. Thank you again and God bless !
Cmiiw : SA node -> AV node -> Bundle of Hiss -> Purkinjae Fibers
Location,
SA : Crista Terminalis - Atrium Dextra Posterior
AV : Trigonum Koch - near A-V Valve
Bundle of Hiss : Interventriculare Ceptum
Purkinjae Fibers : spread in Miocard Ventricle
Need videos on heart failure, CAD, rheumatic fever, IHD
I wonder what
sort of student are you and if you have got qualification which is verified by those who are well qualified in this subject not necessarily a doctor or a professor ?
What's the relation between the first and second graph?
diastole should rightly pronouns as di-as-to-le or as di-as-tole. please let me know.
He mispronounced "systole" and "diastole". It should have sounded like "sis-TOE-lee" and "die-ASS-toe-lee". I came to the comments section to see if anyone else noticed that and you were the only one!
I'm so happy I saw this video !!! I'm very grateful, thanks so much it was excellent an so are you. Life will multiply you good actions !!!
Thank you very much for this vid.
I'm just in awe. lol. such skill going on here. thanks for the video!
you are amazing!! my college professor is no where as clear as you are. it took 2 classes to cover this subject and you did it in less than 30 min.
very very very very ......... Great work , u have a genius creative mind (prefrontal cortex :P ) that connects all things together in a simple way ,,, I really love this way of looking at things
thanks very much man , u are a hero :D
great vid, keep em coming, just please make sure everything youre writing/saying is correct by reviewing your work
May i know what reference book/s you are using kind sir?
After the T wave, you said the ventricles start filling but your wrote "arterial diastole" i am bit confused :/
HALP!
Did you get your answer. I'm confused too!
@@muskansood6363 i think he wanted to write ventricular diastole and was just a typo
@@muskansood6363 i think he wanted to write ventricular diastole and was just a typo
ok...one question right,,,for the ventricle graph..first depolarization means filling the with positive charge..so how is phase0 systolic when there is rapid depolarization....could you kindly explain that as soon as possible
Mr. Richard Adetoye, there's no reply option to your comment so I'll just answer you question here. When you mean systolic, there is contraction of ventricular muscles to push the blood from the ventricles to the pulmonary artery or to the aorta. Depolarization means making the membrane potential to become more positive to make muscle contraction possible. Phase 0 means depolarization of the ventricular muscles thus is part of the systolic phase. Hope this helps.
if you look into the period of the cardiac cycle, there is about 0.3 sec when four chambers are all relaxed and waiting for blood coming into the atrium.I think that area should be shown longer. thank you!
you have saved so many lives with your videos i hope you know that!
thaaaanx it made alot of sense now..ive been looking for the video next to this one but i couldnt find it could u please tell me how to find it..many thanx
Did you make th video explaining whats going on with the heart (visually) when looking at the ECG?
Hi, good catch when you said atrial diastole instead of ventricular diastole. But if you want to add in, the S4 sound should be heard right before the QRS complex. Also when you drew the cardiac myocyte action potential on top of the EKG, shouldn't phase 3 include the T wave instead of ending at the T wave, since the T wave represents ventricular repolarization.
Is the bundle of his the same structure as bachman bundle, or is it different? Thank you!
I can’t explain my feelings for ur explanations!
Just can tell you u are gorgeous ✨
I love you man
I request that please during delivery of your lecture you are too fast.so please reduce your speed
Diastole doesnt mean filling... it means expanding in Hellenic. Furthermore, systole means contraction, also in Hellenic language (Greek)
ruclips.net/video/gplKCkQe7qc/видео.html
I love you so much man....keep impressing me Armando 💖
Watched whole videos from the top of Himalaya to ease through the medical exams.bravo
Okay i have a conceptual doubt, you said that in SA node, repolarisation by efflux of Potassium is followed by depolarization of the next Action Potential Cycle. But how do the Calcium ions which entered the cell in the previous cycle go out? Thats a necessary step before the next cycle begins isn't it? Please help me with this i always struggle at this part. :(
He answered it at around 10:20 of the vid. :)
+Claire De Guzman true
This is probably a minor and inconsequential point, but at ~8:50, Armando mentions phase 0 (the steep upward curve) and states that the influx of sodium is the contraction of the ventricles. While this phase of the action potential is the depolarization of the membrane, the voltage-gated influx of calcium (Ca) ions (via the L-type channels) starts at about -40 mV and is more prolonged than sodium influx (lasting throughout phase 2). The Ca ions which influx during this phase trigger a massive release of Ca ion storage from the sarcoplasmic reticulum, which is responsible for ventricular contraction. Therefore, I believe it would be more precise to say contraction of the ventricles happen during phase 2. Source: Pathophysiology of Heart Disease, L. Lilly.
hey man great video. I just have a quick note about the SA node phases. In phase 4, it is true that the L and T types open up channels but they do so after it reaches -40 mV. From -55 to -40 mV is produced by something called a funny channel which is activated by negative membrane potential and this channel bring in Na +. Just wanted to add detail but great video, love your stuff please keep doing what youre doing!
Yes you're right
Yes that's true there are funny channels envolve here
What's the difference between spontaneous depolarization and depolarization on the first graph,?
so does R correspond to the first heart sound, and T the second heart sound?
Just one question, in the explanation about the cardiac muscle cell contraction, you say that Na+ stop moving in in phase 1, but then in phase 3 you say both Calcium AND sodium stop moving in, how can the sodium influx stop twice ?
you can't imagine how thankful I am... my exam is tomorrow and I was crying cause I didn't understand it till I found your video and it appears clear like water... thanks you so so much!!!!!!❤❤❤❤❤❤❤❤❤❤❤
I enjoy watching the VERY informative videos. Do you have one about the pericardium anatomy?
The videos are just amazing and so to the point..also Please post some detailed videos on CARDIAC ARRTHYMIAS and ANGINA PECTORIS..and if it has already been made..please provide the link..unable to find it..
what if we translate your videos to other languages so they can be available on the captions of the video??? :D
This is the first time this has made sense to me - many thanks!
Beautiful artwork!
I graduated school because of the videos on RUclips just write notes and study these examples I am a licensed EKG Technician
Been struggling to understand this for my A&P exam.
Im so happy i found your channel again.
Subbed so i never lose it again xD
grt diagram it explain and cover all ...bt u can even make it simplier..
So much clearer than the school lecturer. Did not understand anything before watching your videos.
Where is the video for the cardiac cycle???
where do you teach? I love your videos , you are very good.
+zachy pembleton lmao i guess he's ganna have two new students
Armando gets zero hate comments. Whoever comes here goes away with clear concepts.amazing teacher.thank you sir ♥️
Very nice videos; kindly make a video on EKG also.
Thanks.
Very nice video. Especially lining up ECG with contractile cycles (systole/diastole)
Thank you so much for helping students like me. Only searching for good teacher 🙂
You don’t say where blood goes when it leaves heart,two exits?
I think you are so skilled
thanks for all those videos you make ...they helped me a lot .. perfect as a study guide
What what that by which u erased the marker
Ok... so.maybe I am getting confused between skeletal and cardiac. But wouldn't a repolarization involve an influx of potassium? He says eflux but this doesn't make sense to me cause the whole purpose of membrane potential is offsetting balance between sodium and potassium and a continued eflux of potassium would never allow the membrane to reach resting membrane potential. Thanks
Hey sorry if I'm wrong but what I think is this: Depolarization --> 3 Na influx & 2 K outflux, thus the inner side of the cell membrane becomes more positive resulting in depolarization.
Repolarisation means that the inner side of the cell membrane has to become more negative. So we have to pump extra positive charge out of the cell, this way we get a negative inner side of the cell membrane.
Thus the Na-K pump pumps 2K out of the cell...K efflux. Hole it helps. :-)
*Hope. The Na-K pump only pumps Na out of the cell and K into the cell. It's a one way pump. Search: Na-K pump conformations. Being in a particular shape of the pump E1 or E2 creates specific affinities to either K or Na. I think, please google and tell me if I'm wrong, that on the inside it can only pump Na inside and K outside.
I'm not sure if I get you question right, but when you say repolarization, you are making the inside of the cell more negatively charged. For you to be able to do this, Ca2+ and Na+ channels should be closed to prevent further increase of positive ions within the cell, and also, there must be a K+ eflux so that positive ions will move out of the cell making it more negative thus repolarizing it.
Your lectures are amazing!!!!
Sir
When are you uploading Next Video on this topic..??
thanx for providing the image...And for everthing else.. :)
K+ efflux is by voltage gated or leak channels?
Thank you for this amazing video but i want to point out about the action potential of the SA node, the action potential peak reaches +10 not 0, otherwise there will be potential difference between the charges if it stops at 0
the "HAWT" LOLZ!
This man's vids saves me in Physiology. Thank you so much.
What's the mechanics behind calcium in systolic arrest?
Ucan draw!!&U know the material 😋 thankU 4 sharing💖
How calcium blockers affect the normal function of heart?
I'm watching most of your videos are really helpful thank you so much
Thank you so much for doing these man! Absolutely fantastic as a study guide!
i hope you're not busy, but i really need the "NEXT" video as soon as possible. Thank you so much for all your other videos, you're really great!
GRACIAS
Nice vid thanks man, m trying to relearn all this stuff
This video is really well done and explained, thank you very much my friend
Congrats for such a good vid, nice electrocardiographic correlation!
Sir u r amazing... Love from India!!!!
your videos really helped.I have a question now, what is the blood flow from the coronary sinus to the femoral artery? thanks in advance
Check on google.
this is good armando
very very helpful ! thanks for d tutorial !
WHY ITS SO CONFUSING
God Bless you I ThanksGod tour Life
Thank you a lot. This makes clear all the confusion I got with books.
can you make a video on cardiac cycle please
There is something not clear to be , when you draw a digram of ECG how it can be the distend from P wave to R represent atrial systole ( ventricular diastole ) and the distend from the T wave to P wave atrial systole also. Please if you can make it more explanation to me . Thank you
Mosbah Maryd The atria are in diastole most of the time - atrial systole only occurs during the PR interval.
Action potentials fire first which causes the muscle to contract. We start with the heart relaxed, with the atria and ventricles in diastole, both full of blood.
The action potential spreads across the atria (P wave) then there is a small amount of time, about 0.2 seconds, before the action potential reaches the ventricle muscle cells (QRS). This small amount of time is called PR interval, and during this time the atria contract, squeezing their blood into the ventricles (atrial systole), and then relax (atrial diastole) and repolarise. The atrial repolarisation can't be seen on an EEG because the action potential (QRS) reaching the ventricles is so much stronger.
During the time between S and T, the ventricles contract (ventricle systole) and pump blood into the lungs/body. Ventricles then relax (diastole) and repolarise. The T wave is ventricular muscle cells becoming more negative so they are ready to contract again for the next heart beat. The entire heart is resting in diastole during the time between T and the next P.
Mosbah Maryd
Thank you so much
thank you
Thank you soooo much🙏🏻
Your hand is amazing
Good! But can you also tell us about "Renal vascularization"?
great video, thank you for taking the time to post this material it has been very helpful.
The greatest!
Pleases make a next video to this
How to left atrium contract???