Very useful info. Great how the instructor has such a command over the topic. His 14 minute video is more informative than the $100 book I have for the course!
I was soooo lost during our ECG lectures. I am coming to this channel to help prepare because our professors are doctors that see this everyday. Something simple to them is complex for someone new .
Hi team, love your videos. On these ones, it’s hard to follow where Zac is pointing unless he either specially says which strip he is on, draws on it or makes his pointer bigger. Eg R-R intervals (1:51) couldn’t see how he calculated it. Always love your work and you’re the best
Thanks Zacj.. regareding junctional rhythm.. i did not see any wide QRS complexes, yet as long as it is junctional it should be narrow.. kindly clarify?.. Regards
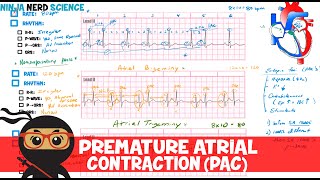
1. Rate: normal, tachycardia, bradycardia 2. Rhythm - R-R interval: regular - P wave: sinus (II +, aVR -)[if inverted: lead misplaced, dextrocardia, ectopic rhythm], ectopic (atrial ectopic rate > 60 abnormal p wave or retrograde), junctional (AV node rate 40-60 might be retrograde p wave too cause might be SA node damage), idioventricular (Purkinje fibers rate 20-40 looks like PVC also it might be accelerated to a rate of 60) - P -> QRS: AV association, heart block, AV dissociation (if no p wave then it is dissociation) - QRS: narrow, wide (VT, junctional rhythm) PVC due to hypoxia, electrolytes abnormalities, increased sympathetic nervous system activity. Looks like idioventricular wave.
i love the work u guys do. U guys have helped me a lot throughout the years. just a quick favor. Could you talk more about skeletal and integuementary. Skeletal, specifically the physiology of like functions as well as ossification
Thank you so much Ninja group plz next episode I would request to be acute kidney injury, chronic kidney injury and glomerulonephritis Thank from Somalia
Very good explanation 😍 but zach, i think that i see 2 waves afer the QRS complexes in the first EKG, i think that it's a T wave and a retrograde P wave!
I learned alot as usual. My question is, how would you different a junctional escape rhythm from a ventricular escape rhythm if both of them are at 40bpm since they have similar features and cut across 40bpm?
I m not sure , but in the most cases a jonctional rhythm has narrow QRS because the impulses will be still conducted on the fast physiological pathway ( Hiss-Purkinje system) while a ventricular escape rhythm will have broad QRS. There are cases when a jonctional rhythm is associated with large QRS ( when is combined with a bundle branch block). In this case you will make the difference between jonctional and idioventricular rhythm according to previous ECG-s of that patient when he had sinus rhythm
Why’d you calculate 90 bpm with lead II in the top right and then calculate 50 in lead III? And there’s two lead II’s? Super appreciative of the videos. Gladly a patreon supporter.
And when you determine the width of the QRS, it sounds like you are pointing out something on the ECG but I can’t see where you are referring to. Thanks!
@@joshcrane4107 in his previous ECG he taught about 10 second strip and 6 second strips to calculate the beat 🤔 he also did it box by box just to check the range, so long as it’s within the range he’ll take it into consideration
Kristine Kwan thanks. But there’s two lead II strips. I guess that’s my confusion. The box method and three hundred rule are straight forward. But I’ve never seen someone calculate HR from two leads. In medical school, I believe I was taught to calculate the HR with lead II with the 300 rule. Just trying to clarify where the strip in the top right came from. Thanks!
Thank you so much for your support! The top right ECG is completely different. Please don’t get this confused with the 12 lead strip. We included the top right rhythm strip as an opportunity for extra practice. Thanks!
And, can we have multiple ectopic foci simultaneously, and if yes, what would be it's manifestation on EKG, and would it differ based on the distance between the ectopic foci's?
Dr. Zach Murphy, can we have multiple pacemakers working simultaneously, like any two or more of (SA node, AV node, ectopic focus or Purkinje fibers) firing together?
how do i differentiate between atrioventricular ,junctional and pvc ??? someone help please cause the only difference i see between them is the rate but at the end he said it also might be accelerated. so how do i differentiate ?
I don't see wide QRS in this video. They are less than two small boxes. Seems like your theory it is junctional influenced how you characterized the width of the QRS complex.







![BLACK BAG - Official Trailer [HD] - Only in Theaters March 14](http://i.ytimg.com/vi/Du0Xp8WX_7I/mqdefault.jpg)

You are the best teacher of this material I've ever learned from.
Very useful info. Great how the instructor has such a command over the topic. His 14 minute video is more informative than the $100 book I have for the course!
I was scared you were gone forever. Thank you!!
Hands down best EKG video ever
Amazing new style of explanations, may god bless your efforts 💚
Oh yeah after five months l am here really to study them 💚📒📚
Ninja nerd saving my medical career one video at a time
Loved it. It feels like medical is field where u hv to figure out everything on ur own. But here its different vibe😍!
I was soooo lost during our ECG lectures. I am coming to this channel to help prepare because our professors are doctors that see this everyday. Something simple to them is complex for someone new .
Thanks!
You guys are amazing. Ive told all my friends about you.
Hey!, Thanks, I've been waiting for this series of vedios.
Hi team, love your videos. On these ones, it’s hard to follow where Zac is pointing unless he either specially says which strip he is on, draws on it or makes his pointer bigger.
Eg R-R intervals (1:51) couldn’t see how he calculated it. Always love your work and you’re the best
exactly guys olease use a darker colour when pointing or writing on the ecg
Awesome explanation GOT IT will be ready for my EKG test for work
Thanks Zacj.. regareding junctional rhythm.. i did not see any wide QRS complexes, yet as long as it is junctional it should be narrow.. kindly clarify?.. Regards
I was thinking “ am I the only one that noticed QRS is not wide ? “
Same
1. Rate: normal, tachycardia, bradycardia
2. Rhythm
- R-R interval: regular
- P wave: sinus (II +, aVR -)[if inverted: lead misplaced, dextrocardia, ectopic rhythm], ectopic (atrial ectopic rate > 60 abnormal p wave or retrograde), junctional (AV node rate 40-60 might be retrograde p wave too cause might be SA node damage), idioventricular (Purkinje fibers rate 20-40 looks like PVC also it might be accelerated to a rate of 60)
- P -> QRS: AV association, heart block, AV dissociation (if no p wave then it is dissociation)
- QRS: narrow, wide (VT, junctional rhythm)
PVC due to hypoxia, electrolytes abnormalities, increased sympathetic nervous system activity.
Looks like idioventricular wave.
Great job, zach and team!
And for you who read this comment, have a good day!
The best in everything, thank you!!
We love you ninja nerd ❤️
i love the work u guys do. U guys have helped me a lot throughout the years. just a quick favor. Could you talk more about skeletal and integuementary. Skeletal, specifically the physiology of like functions as well as ossification
Excellent explanation. I will support next time practically by donating some.
Thanks a lot! Your videos literally saved me
Excellent! Would appreciate information on how to treat these disrythmias as well 😀
So helpful. Thanks Zach!
You are the best 👍
Thank you! This is helping so much!
Thanks ninja nerd 🙏🙏🙏
amazing explanation thank you so much!
thank you thank you for all you do!
I really love your videos! Keep up the good work :)
@2:50 what is the purpose of checking aVR after lead II, if there is no p wave in lead II?
Thanks Prof God bless you
Thank you as always
The ECG and the rhythm strip you used are different. They have completely different rates. Why would you do that?
Was wondering the same thing
thank you so much for everything ❤️❤️❤️❤️
super helpful, thanks
Congratulations 300k subs
Nicely explained
Thank you so much Ninja group plz next episode I would request to be acute kidney injury, chronic kidney injury and glomerulonephritis
Thank from Somalia
Very good explanation 😍 but zach, i think that i see 2 waves afer the QRS complexes in the first EKG, i think that it's a T wave and a retrograde P wave!
I was wondering the saaammmmeee!!!
I learned alot as usual. My question is, how would you different a junctional escape rhythm from a ventricular escape rhythm if both of them are at 40bpm since they have similar features and cut across 40bpm?
I m not sure , but in the most cases a jonctional rhythm has narrow QRS because the impulses will be still conducted on the fast physiological pathway ( Hiss-Purkinje system) while a ventricular escape rhythm will have broad QRS. There are cases when a jonctional rhythm is associated with large QRS ( when is combined with a bundle branch block). In this case you will make the difference between jonctional and idioventricular rhythm according to previous ECG-s of that patient when he had sinus rhythm
@@alesandro-gabrielbuhusi7342 Thanks for the in depth answer my friend.
@@Sk1pperCS You're welcome
Good job 👏 thanx 💜
Why’d you calculate 90 bpm with lead II in the top right and then calculate 50 in lead III? And there’s two lead II’s?
Super appreciative of the videos. Gladly a patreon supporter.
And when you determine the width of the QRS, it sounds like you are pointing out something on the ECG but I can’t see where you are referring to. Thanks!
@@joshcrane4107 in his previous ECG he taught about 10 second strip and 6 second strips to calculate the beat 🤔 he also did it box by box just to check the range, so long as it’s within the range he’ll take it into consideration
Kristine Kwan thanks. But there’s two lead II strips. I guess that’s my confusion. The box method and three hundred rule are straight forward. But I’ve never seen someone calculate HR from two leads. In medical school, I believe I was taught to calculate the HR with lead II with the 300 rule. Just trying to clarify where the strip in the top right came from. Thanks!
Thank you so much for your support! The top right ECG is completely different. Please don’t get this confused with the 12 lead strip. We included the top right rhythm strip as an opportunity for extra practice. Thanks!
@@NinjaNerdOfficial U r missing in these ECG videos sir !!.
ExcellentI Thank you>
but what's the difference between the 2 on the ecg?
Are the atria contracting in junctional & idioventricular rhythms? And is the stroke volume reduced?
Junctional can be 40 BPM also though, how do you differentiate other than rate?
Please we need vedios of molecular biology
And, can we have multiple ectopic foci simultaneously, and if yes, what would be it's manifestation on EKG, and would it differ based on the distance between the ectopic foci's?
Thanks for education ninja group and zach .please teaching enzymology I need your help very .please!! Thank you🙏🙏🙏
Amazing
Plz make the videos on topics related to molecular biology, genetic engineering and biotechnology in detailed
thank you so much
sir we are getting difficulty in dermatology. we request you to make video on it.
I am requesting you to make videos on Bioinformatics . We need this very much. Please!!!!!!
Thanks
VERY NICE
Please do videos on laryngeal system..
Awesome
Dr. Zach Murphy, can we have multiple pacemakers working simultaneously, like any two or more of (SA node, AV node, ectopic focus or Purkinje fibers) firing together?
there is 3rd degree av block which sa and av node works seperately
MAT
Thank you
how do i differentiate between atrioventricular ,junctional and pvc ???
someone help please
cause the only difference i see between them is the rate but at the end he said it also might be accelerated. so how do i differentiate ?
Signal boost comment 🤙🤙🤙
I don't see wide QRS in this video. They are less than two small boxes. Seems like your theory it is junctional influenced how you characterized the width of the QRS complex.
I thought that when it is Junctional Rhythm QRS is narrow, and if it is Idioventricular Rhythm QRS is wide
Sir I love you
thankyouu
תודההההה
Can't see the top of your screen.
Wizard.
❤❤❤
❤
🌹
thinks
💯🥷💯🥷💯
Annoying
Thanks!
Thanks
❤❤❤❤❤