Thanks for watching! Please subscribe and join Dr. Seheult for the rest of the ECG video series at: www.medcram.com/courses/ekg-ecg-interpretation-explained-clearly
Are you a professor at Harvard university? If not, I think you should because you are amazing!!. This is what the students need in college. A first class professor. Thank you
This makes me want to become a doctor. 36 years old, AEMT, highest schooling is Associate Degree. No time like the present. Any ideas on which Bachelor degree would help me the most for getting into Med School would be greatly appreciated!
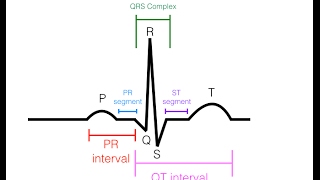
Hello! I am not sure if I understood correctly, you said around 8:01 that the R wave is the positive component and S is the negative, but S is always after R. Wouldn’t that be the Q wave of necrosis?
I do speach analysis and work with models to filter noises and recognise words. Can the medical field not feed these ECG readings to a machine that can quickly diagnose and report?
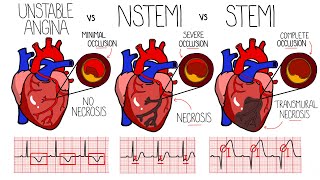
st segment depression in avr +tachycardia= percarditis but in other video u said a lot of st segment elevations...almost in every lead...is seen in pericarditis...?
St elevation has many differential the diagnosis is based on the full clinical presentation not ECG Alone in pericarditis you need 2 out of 4 following criteria •Typical Chest pain (sharp, pleuritic improve by sitting up and lean forward) •pericardial friction rub •suggestive ECG changes (wide spread ST elevation with reciprocal ST depression in lead AVR and V1 •New or worsening pericardial effusion on ECHO hope that answered your Question




![Noob To Max With DRAGON REWORK In Blox Fruits [FULL MOVIE]](http://i.ytimg.com/vi/LnBMOinoOvA/mqdefault.jpg)
![I.N "HALLUCINATION" | [Stray Kids : SKZ-PLAYER]](http://i.ytimg.com/vi/n5B5q1Hwt_U/mqdefault.jpg)


Thanks for watching! Please subscribe and join Dr. Seheult for the rest of the ECG video series at: www.medcram.com/courses/ekg-ecg-interpretation-explained-clearly
Sir , no one teaches us the way you taught here. Thank you very much
Are you a professor at Harvard university?
If not, I think you should because you are amazing!!. This is what the students need in college. A first class professor. Thank you
Thank you for the feedback!
I was struggling to freshenup my memories of ECG and you made it really simple,better that how i studied it even. Thank you so much.
I appreciate your effort putting out the video.
Perfect explanation, concise and very informative!
soo good.
thank you so much for making videos like these. :)
This makes me want to become a doctor. 36 years old, AEMT, highest schooling is Associate Degree. No time like the present. Any ideas on which Bachelor degree would help me the most for getting into Med School would be greatly appreciated!
Hello! I am not sure if I understood correctly, you said around 8:01 that the R wave is the positive component and S is the negative, but S is always after R. Wouldn’t that be the Q wave of necrosis?
good review while I am on call for the cathlab! lol...trying to keep occupied for the next 3 days of call..
You lost me on the Axis explanation 😫
So good... Thank you!
Nice
Thank you very much
The way you explained the axis was quite difficult,sorry.👍🙄
I think u explained well, but I can't understand anything, nursing student 😊
Many thanks.
why do we have to do another EKG ?????????????
I do speach analysis and work with models to filter noises and recognise words. Can the medical field not feed these ECG readings to a machine that can quickly diagnose and report?
Very nice, consise presentstion
One thing only can you please move the writing up or down because we can't see the explanation drawing
Thanks
WELL DISCUSSED CASE
Thank you. Can you please have a lecture about Type 2 MI vs. myocardial injury? I am not in Medical field but still I enjoy learning.
Thanks sir
Nice information
st segment depression in avr +tachycardia= percarditis
but in other video u said
a lot of st segment elevations...almost in every lead...is seen in pericarditis...?
St elevation has many differential
the diagnosis is based on the full clinical presentation not ECG Alone
in pericarditis you need 2 out of 4 following criteria
•Typical Chest pain (sharp, pleuritic improve by sitting up and lean forward)
•pericardial friction rub
•suggestive ECG changes (wide spread ST elevation with reciprocal ST depression in lead AVR and V1
•New or worsening pericardial effusion on ECHO
hope that answered your Question
O