Pediatric Hyperkalemia

HTML-код
- Опубликовано: 8 сен 2024
- Homepage: EMNote.org ■
🚩Membership: tinyurl.com/jo...
🚩ACLS Lecture: tinyurl.com/em...
Pediatric Hyperkalemia
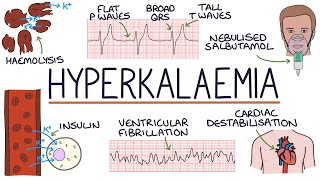
Hyperkalemia is less prevalent in pediatric patients compared to hypokalemia. However, hemolysis in patients who undergo heel stick lab work is not uncommon. The cutoff for determining hyperkalemia is contingent upon the age of the patient. Typically, levels up to 6.0 mmol/L are well-tolerated in children, unless the shift is rapid. Any child meeting age-related hyperkalemia or who has a known lower prior potassium level should receive an electrocardiogram (ECG).
Mild to moderate elevations (below 6 mmol/L) in serum potassium concentration are typically asymptomatic in children. However, as the potassium exceeds 7 mmol/L, the risk of life-threatening clinical manifestations increases rapidly. Rarely, rapid increases in serum potassium above 6 mmol/L may cause signs and symptoms in high-risk children.
Hyperkalemia is caused by an excess of total body potassium or by the increased movement of potassium from intracellular to extracellular spaces. In contrast to hypokalemia, insulin deficiency and acidosis allow potassium to move extracellularly. Unique to hyperkalemia are causes of cell injury that allow intracellular solutes, including potassium, to flow into the extracellular space. Any source of cell injury or lysis in children can cause hyperkalemia.
Hyperkalemia is diagnosed on routine electrolyte testing. Before extensive evaluation of the cause of hyperkalemia, it is critical to assess the child for cardiac or neurologic symptoms or for risk of developing signs and symptoms. An ECG should be obtained urgently in these cases. Once the patient has been stabilized or the potassium level lowered to a safer range, further evaluation must be performed to identify the cause of the hyperkalemia.
A child with symptomatic hyperkalemia (including concerning ECG changes) or a potassium concentration greater than 7 mEq/L (7 mmol/L) represents a medical emergency. The goal of treatment in these patients is to lower the serum potassium level to prevent life-threatening arrhythmias. No matter the underlying pathology, treatment in this case involves decreasing the total body potassium load and moving potassium intracellularly. All nutrition, fluids, and medications containing potassium should be discontinued. Medications that move potassium intracellularly include insulin (administered with glucose to prevent hypoglycemia), β-agonists (albuterol, terbutaline), and bicarbonate (noting that in the absence of acidosis, the role of bicarbonate to treat hyperkalemia is unclear). Simultaneously, efforts should be made to lower the total body potassium level with loop diuretics (furosemide, bumetanide).
Treatment for hyperkalemia is similar to that in adults. Calcium chloride (20 mmg/kg - max 1 g) or calcium gluconate (0.5 mL/kg - max 20 mL) is given for cardiac stability. Albuterol can be given based on weight. Insulin and dextrose can be used with extreme caution and close monitoring for hypoglycemia. If hypoglycemia occurs, dextrose should be given as D10% in children younger than 5 years of age; D25% can be used if the child is older than 5 years.
Key differences between hyperkalemia in adults and in children:
In adults, common causes of hyperkalemia include kidney disease, diabetes, medications (e.g., ACE inhibitors, potassium-sparing diuretics), and severe tissue injury.
In pediatrics, dehydration, metabolic acidosis, and congenital disorders (e.g., renal tubular acidosis) are more common causes.
Typically, levels up to 6.0 mmol/L are well tolerated in children, unless the shift is rapid.
Symptoms may be less specific in children, which include irritability, lethargy, and gastrointestinal disturbances.
The use of insulin and glucose is more cautious in pediatrics due to the risk of hypoglycemia, and alternative agents like albuterol may be considered. Diuretics are used cautiously in children due to the risk of dehydration, and dialysis is often required for severe cases.